There is currently no consensus in the medical community on the utility of intravenous (IV) saline in people with postural orthostatic tachycardia syndrome (POTS). Some physicians will prescribe it for acute hypovolemic shock (discussed below), but not for regular long term care, for a variety of reasons. Other physicians will prescribe daily or weekly use of IV saline in treatment of POTS in some patients. Some use IV saline 24/7 using a battery operated pump in a backpack. Many people with POTS will use a PICC line or port a couple of times a week for a liter or two of saline.
Intravenous saline is used to treat significantly low blood volume, which can be a problem for some people with POTS. This can be difficult for doctors to test because it is a ratio of red blood cells to plasma volume. In POTS, both the number of red blood cells and the plasma volume can be low (and thus the ratio appears normal on the CBC). For some with POTS, their blood levels can drop low enough to result in hypovolemic shock. The best way to get a measure of your blood volume is to do specific blood volume testing which uses a radioactive tracer called iodinated-RISA. The tracer is injected using an IV and then blood samples are taken over time to measure the tracer levels in your blood and determine your blood volume.
Symptoms of hypovolemic shock:
- Anxiety
- Blue lips/fingernails
- Chest pain
- Confusion
- Dizziness
- Loss of consciousness
- Low blood pressure
- Low or no urine output
- Profuse sweating
- Shallow breathing
- Tachycardia
- Weak pulse
Be sure that you speak with your doctor about methods to increase and/or maintain your blood volume. There are several ways to increase your blood volume naturally, and these should be explored before considering IV saline as a therapy for low blood volume. The most common treatments used by people with POTS are increasing salt and water consumption. Exercise is also a great way to increase blood volume. There are also medications that can help with blood volume expansion (e.g., Florinef, midodrine).
Why might IV saline be better than oral fluids? In some cases, nausea and vomiting when drinking liquids defeats the purpose and can severely limit fluid intake. In others with rapid gut motility, less water is absorbed into the body than normal as it is rushed through the intestines. In addition, if your blood volume is low, but the ratio between red blood cells and plasma is normal, you may not be able to absorb the fluids even if you are drinking several liters per day.
Why use IV fluids? Intravenous fluids bypass the digestive tract to eliminate issues with nausea/vomiting and gut motility. The saline goes directly into your bloodstream to increase the plasma volume. In fact, a liter of normal saline can reduce both heart rate and other symptoms like brain fog in a person with POTS if her blood volume is low.
The main barrier in using IV fluid therapy is accessing the bloodstream. When a person has low blood volume, their veins tend to be small and difficult to access. The decision to use regular IVs, PICC lines, and ports must be made with your doctor and depends on a number of factors.
- Do you have good veins for access when using a regular IV?
- How long do you foresee needing regular IV saline therapy?
- Would you be comfortable accessing a line at home by yourself or with a family member? If so, would insurance pay for home access?
- Are you using IVs for medications other than normal saline?
- Before getting a PICC line or port, have you tried using IV saline regularly for a few weeks to be sure it helps your symptoms?
Peripheral Venous Access (Regular IV)
These are the traditional IVs that are accessed via veins in the arm, hand, neck, or feet. They stay in the periphery and never approach the superior vena cava or the heart. The tube that fits into your vein is generally less than two inches long and can be placed by most nurses. These work well for those with good veins who need infrequent access (once a week or less) to IV fluids. Regular IVs are inexpensive and can be easily placed and removed. The downside to regular IVs is that you must go to the ER, doctor’s office, or an infusion center to get IV saline.
If you need to go to the Emergency Department for IV saline, consider printing this sample letter and discussing it with your doctor. If your doctor will modify this and put it on letterhead, you could carry it with you when you have to visit the ER for IV fluids.
Central Access Devices
All of these devices will be placed into the superior vena cava, a large vein that leads into the right atrium of your heart. Both implantable ports and peripherally inserted central catheters (PICC) are central access devices. Consider talking with your doctor about a PICC line or a port if you have been getting infusions more than once a week for at least 6 months.
Central access devices can be used to give long term medicine treatment for pain, infection, or cancer. They can also be used to deliver nutrition or large amounts of blood or fluid quickly. In addition, these devices can allow frequent blood samples without having an additional “stick.” In most people with POTS, these lines are used mainly for administration of saline therapy.
These devices can be accessed by professionals at an infusion center or by you and your family at home. For many people with POTS, the ability to get IV fluids at home when starting to go into hypovolemic shock can improve overall quality of life and help make life more predictable by stopping flares quickly.
Implantable Ports (Power Port, Mediport)
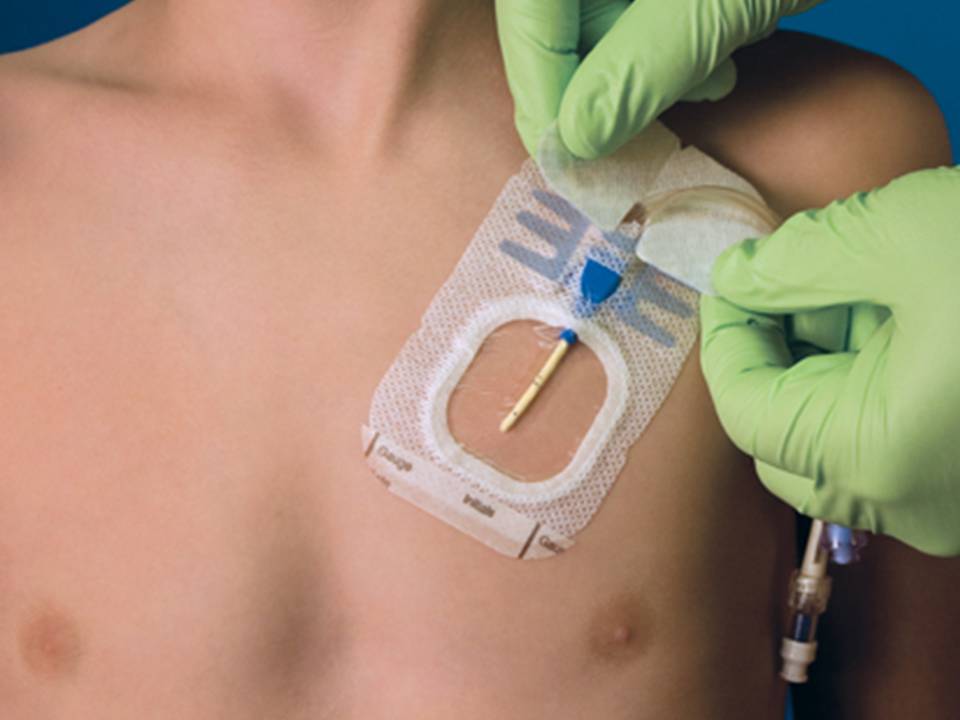
- A hub is placed into small pocket under the skin below the collarbone and the tube runs from the hub into the superior vena cava. You access the port through the skin with a special needle. You can use a topical numbing agent to minimize feeling the “stick.”
- Pros
- Can be used to get fluids at home
- Can be left in your body for years
- Requires dressing only when accessed
- The needle can stay in the port for up to a week
- Best for intermittent use
- More permanent than a PICC line
- Once healed, the port site does not need to be kept dry
- Can shower, bathe, and swim with a port once it is healed
- Cons
- Placement requires surgery and anesthesia. It is usually placed by a general or vascular surgeon in the operating room
- Surgical removal when you are finished with it or if complications arise
- Requires sterile environment and dressing while accessed
- Requires skilled nursing or training to access with needle.
- Can be accessed 2000-2500 times which typically allows use for a couple of years
- Must be flushed with saline and heparin every six weeks
Peripherally inserted central catheters (PICC)
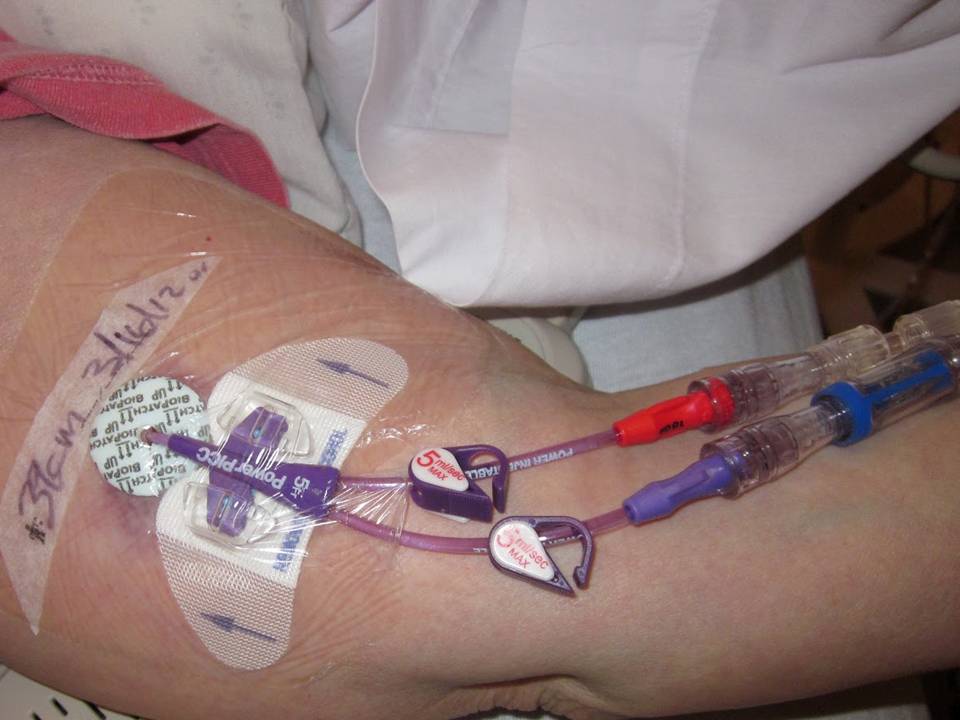
- Inserted into large vein in the arm and threaded through the chest to the superior vena cava
- Pros
- Can be inserted at bedside by specially trained doctor or nurse
- No sedation is required for insertion or removal
- Can be accessed at home for fluids
- Dual lumen PICC allows one lumen for drawing blood and one for IV fluids
- Can be hidden by clothes
- Excellent for frequent access
- Cheaper for your insurance company and perhaps for your co-pay
- Cons
- Short term use: usually kept for three months or less
- Higher risk for deep vein thrombosis (blood clots)
- Must be covered at all times
- Requires sterile dressing that must be changed weekly
- Partially external device
- Higher risk of infection than ports
- Can be accidentally snagged because it hangs out of the arm
- Visible to others
- Must be kept dry at all times
- Can’t swim or bathe with a PICC
- Must wrap and seal it carefully before showers
- Must be flushed daily
Central access devices, both PICC and port, can lead to serious potential complications.
- Blood clots: can form in the veins of the arm and chest. Clots can break away and get lodged in the lungs (pulmonary embolism) which can be fatal. May require anti-coagulants, clot busting drugs, or surgery to correct this problem.
- Bloodstream infection: most common serious complication which requires removal of the line and IV antibiotics. These infections can lead to a systemic infection (sepsis) which can be fatal.
- Perforation of the vein or heart chamber: highest risk during insertion of the line. Rare complication, but has a high mortality rate if it occurs.
- Pneumothorax: highest risk occurs when inserting the line. If the guide wires perforate the lung, air can get into the spaces around the lung (pleural space). This rare complication may require a chest tube or needle decompression to correct.
- Heart rhythm disturbance: occurs when the tip of the device touches the heart wall, resulting in supraventricular tachycardia, premature ventricular contractions, premature atrial contractions, and/or ventricular tachycardia. This usually occurs with insertion, but can also happen with catheter migration or breakage.
- Migration: catheter tip migrates into other blood vessels like the internal jugular vein or mammary veins. This can occur from placement of the device too high in the superior vena cava or vigorous activity, and can cause blockage of the affected veins.
- Pain: you may have pain at the insertion point or where it lies under your skin.
Who is NOT a good candidate for central access device placement? People who should NOT get a PICC or a port include those with:
The following groups would be advised NOT to use a port:
- Poor immune function, as infection is possible
- Factor V Leiden : increases your risk for blood clots and is found in 8% of population
- Antiphospholipid syndrome: increases your risk for blood clots
- Those taking
- Birth control pills
- Corticosteroids
- DDAVP
Reducing the risk of complications
- Doctors should ensure correct tip placement using an ultrasound or other radiology technology. Use of EKG can show disruption of heart rhythm
- Lines placed on your right side have less risk from both perforation and developing clots than those on the left
- Remove the line when it is no longer needed
- Use proper sterile technique when flushing or otherwise accessing the line. Wash your hands!
Call for help when you have:
- Severe trouble breathing
- Sudden chest pain and shortness of breath
- Coughed up blood
- Yellow or green drainage from the device
- Resistance when you inject medicine or fluids into your line
- Signs of infection including
- Increased pain, warmth or redness
- Swelling in your face, chest, neck, or arm on the side of the device
- Red streaks lead from the access site
- Pus or blood is draining from the access site
- Swollen lymph nodes in your neck, armpits or groin
- Fever over 100° F or 38° C
For free, full-length scientific articles on IV saline and POTS, visit Scientific Articles on IV Saline and POTS
For a more personal view of POTS and IV saline options, click here.