POTS Subtypes
Hyperadrenergic, Neuropathic, and Hypovolemic POTS
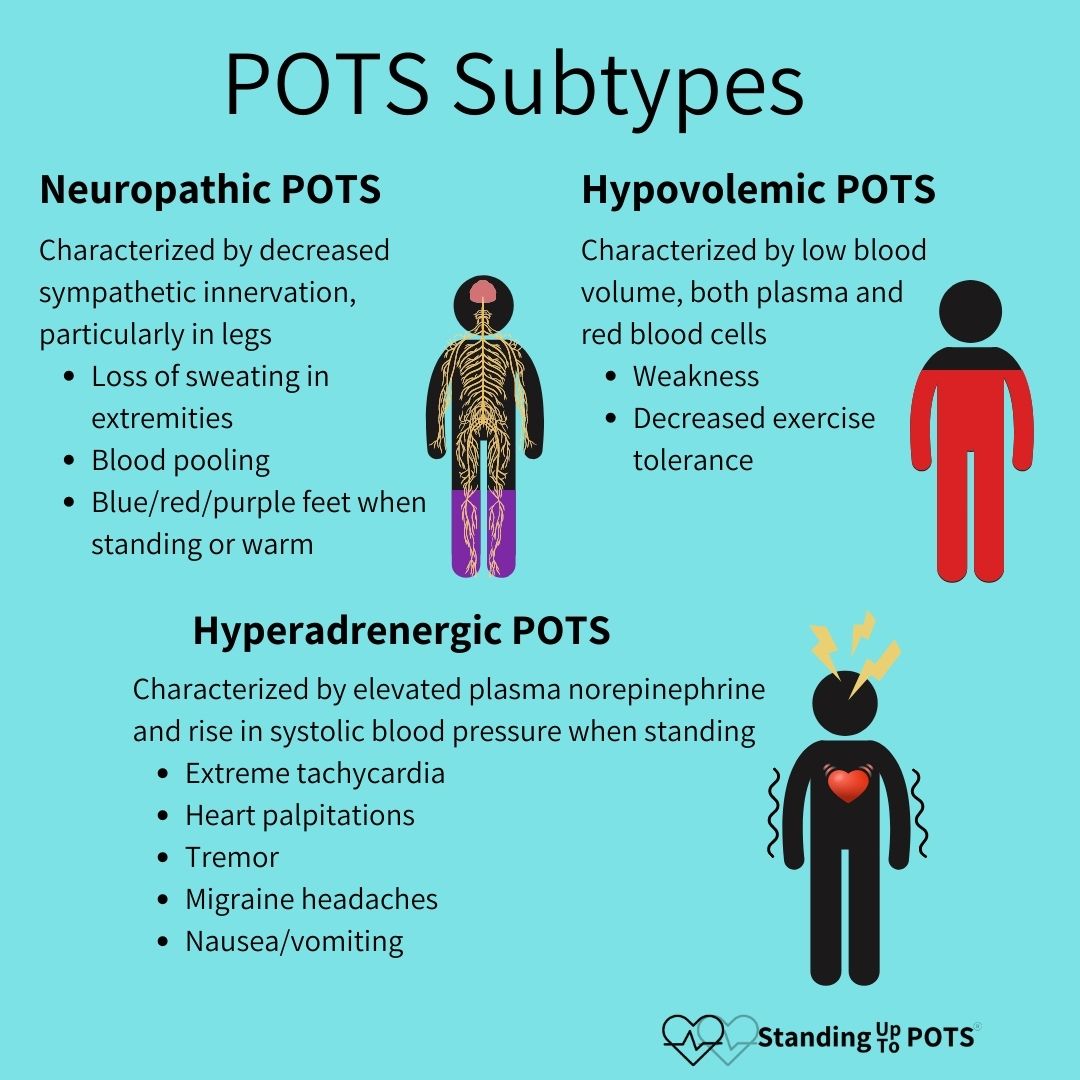
Postural orthostatic tachycardia syndrome (POTS) is the most common form of dysautonomia, characterized by malfunction of the autonomic nervous system. The range of potential symptoms of POTS is broad in both scope and severity. Sometimes practitioners will refer to three subtypes of POTS to help think about the possible mechanism and treatment options. These are not used by all practitioners, so don’t worry if you haven’t heard these terms. There is a lot of overlap between these subtypes: hyperadrenergic POTS, neuropathic POTS, and hypovolemic POTS, and so it is possible that one person could identify with symptoms and taking medications described for each type of POTS. This is common and nothing to be concerned about.
Hyperadrenergic POTS
Hyperadrenergic POTS is characterized by elevated levels of plasma norepinephrine levels (neurotransmitter of the sympathetic NS) >600 pg/mL and >10 mmHg rise in systolic blood pressure while standing for 10 minutes (Low et al. 2009). In hyperadrenergic POTS, the sympathetic nervous system is overactivated.
The most prominent symptoms associated with hyperadrenergic POTS include:
- Increased blood pressure
- Tachycardia that may be more extreme than other subtypes
- Heart palpitations
- Anxiety, tremor, cold, sweaty extremities while upright (Low et al. 2009)
- Migraine headaches
- Increased urinary output after being upright
- Nausea/vomiting
The most common comorbidity with hyperadrenergic POTS is mast cell activation syndrome (Wang et al. 2021). Identifying and treating mast cell activation syndrome, if present, can help to decrease these symptoms. There are a number of other potential causes of hyperadrenergic POTS, which are rare. These include a single point mutation in the norepinephrine reuptake receptor (Lambert et al. 2008), baroreflex failure, and a tumor on the adrenal glands called pheochromocytoma (Benarroch 2012).
Treatments for hyperadrenergic POTS focus on rebalancing the autonomic nervous system, typically by decreasing the activity of the sympathetic nervous system. These medications include:
- Clonidine - central nervous system sympatholytic medication that decreases the central sympathetic tone
- Beta Blockers - block B-adrenergic receptors bound by norepinephrine and prevent sympathetic activity peripherally (Fedorowski 2018).
Neuropathic POTS
Neuropathic POTS is characterized by a decrease in sympathetic innervation, particularly in the legs (Mar and Raj 2020), and is often associated with small fiber neuropathy. Normally, these small fiber nerves regulate constriction of the blood vessels in the limbs and abdomen. Because these nerves are damaged in neuropathic POTS, however, activation of the sympathetic nervous system leads to less release of norepinephrine from these small fibers. Because norepinephrine is a vasoconstrictor, neuropathic POTS is often associated with excessive blood pooling in the hands and feet. This decreases blood circulation and causes less blood to return to the heart (low venous return) which causes the heart rate to increase in order to compensate. Neuropathic POTS often occurs following infection, surgery or trauma and may be an autoimmune form of POTS, as autoantibodies to the ganglionic acetylcholine receptor have been associated with this POTS subtype (Li et al. 2014).
The most prominent symptoms of neuropathic POTS include:
- Loss of sweating in extremities
- Blood pooling
- Cyanosis in the feet (turning a bluish color when standing/warm)
Treatments for neuropathic POTS tend to focus on decreasing blood pooling and moving blood back up toward the heart and brain. These include:
- Graded compression garments, including abdominal compression of 40 mmHg (Mar and Raj 2020) and leg compression of 20-30 mmHg.
- Midodrine – an alpha 1 adrenergic agonist (binds NE receptors) that causes constriction of the peripheral blood vessels and promotes return of blood to the heart and brain (Mar and Raj 2020).
- Pyridostigmine – an acetylcholinesterase inhibitor that increases the acetylcholine levels in the synapse (increasing parasympathetic activity) of autonomic ganglia (Mar and Raj 2020) which helps to decrease heart rate
Hypovolemic POTS
Hypovolemic POTS is characterized by abnormally low blood levels, including both red blood cells and plasma (Raj et al. 2005). While not often measured, the plasma deficit in POTS is approximately 13% and may be related to low levels of circulating renin and aldosterone which typically help to increase blood volume and blood pressure (Raj et al. 2005). As a result, people with this type of POTS have their kidneys excreting too much sodium and water, which contributes to this low blood level. Low blood volume leads to less blood return to the heart, which causes an increased heart rate and force of contraction in an attempt to keep blood circulation at normal levels.
What symptoms are typically associated with hypovolemic POTS?
- Weakness
- Decreased tolerance for exercise
What are the typical non-pharmacological treatments?
- Increased salt (6-10 g) and fluids (2-3 L) to increase blood volume (Fu and Levine 2018)
- Compression garments with at least 20-30 mm Hg pressure, including leg stockings and a pair of biker-style shorts (Fu and Levine 2018)
- Raise head of bed 4-6 inches. Mild orthostatic stress shifts fluid to the lower body which activates the renin-angiotensin-aldosterone system, leading to fluid retention at the kidneys and blood volume expansion (Fu and Levine 2018).
What are the typical medications to increase blood volume?
- Fludrocortisone: enhances sodium and water retention to increase blood volume
- Desmopressin: synthetic version of antidiuretic hormone that increases water reabsorption without increasing sodium reabsorption to increase blood plasma levels
- Erythropoietin: stimulates red blood cell production and increases overall blood volume
- IV fluids can be helpful.
Further Information
Check out this page for more information on medications for POTS that includes dosages and other administration information.
To hear Dr. Cathy Pederson’s episode discussing this topic, listen to The POTScast Episode 88: Three Types of POTS.