Pregnancy in POTS Patients
What healthcare practitioners need to know
Many POTS patients are of childbearing age and may be considering pregnancy. Unfortunately, no consensus guidelines or large clinical trials on pregnant patients with POTS currently exist to use as a guide. Planning a pregnancy for a person with POTS requires preparation in advance to ensure that symptoms can be controlled, the current medication regimen is safe for a fetus, and precautions for comorbidities are addressed.
A POTS diagnosis does not preclude pregnancy. Most young people with well-controlled POTS symptoms and no significant comorbidities don’t have pregnancies that are considered as high risk at this time. On the other hand, people with more severe POTS symptoms, those over 35, and those with multiple POTS comorbidities should be considered “high-risk” and add a maternal-fetal specialist to their healthcare team in addition to the primary care practitioner and obstetrician (Morgan et al. 2022).
Note: we are grateful to Dr. Svetlana Blitshteyn, a leading POTS physician and member of the SUTP Medical Advisory Board, for reviewing this page and sharing her insights with practitioners interested in learning more about POTS.
Normal Physiological Changes that Occur during Pregnancy
During pregnancy, there are significant normal physical changes within the woman’s body to accommodate the growing fetus:
Increased blood volume. The blood volume increases by 45%, with increases in both plasma levels and red blood cell count (Sanghavi and Rutherford 2014). This increased blood volume occurs as more blood is required to nourish the fetus via the placenta and in preparation for normal blood loss during delivery.
Increased cardiac output. Cardiac output represents the number of mL of blood pumped out of the heart per minute. In the first and second trimesters, increased cardiac output is a result of the increased blood volume, which can increase both heart rate and stroke volume (the amount of blood leaving the heart in one heartbeat). It’s normal for the heart rate to increase by 10 to 20 beats per minute from baseline during pregnancy (Sanghavi and Rutherford 2014).
Changes in blood pressure. Early in the pregnancy, there is a normal reduction in blood pressure due to peripheral dilation of the blood vessels from increased levels of the hormones estrogen, progesterone, and relaxin (Sanghavi and Rutherford 2014), which are all vasodilators. By the third trimester, the sympathetic nervous system becomes increasingly active which can help return the blood pressure to normal levels by constricting the peripheral blood vessels (Greenwood et al. 2001).
Pre-Pregnancy: Choosing the Safest Possible Medications
While in most cases it would be ideal to discontinue all medications prior to becoming pregnant, that may not be possible for many POTS patients. It is important to consult with your healthcare practitioner to determine which medications are best to control your POTS symptoms and minimize fetal drug exposure. It may take 6-12 months to transition from current medications to alternatives that control POTS symptoms and are also safer for the fetus. Starting this medication migration before pregnancy is important, as some medications, like stimulants and benzodiazepines, require decreasing the dose over time to wean the patient off of the medication (Morgan et al. 2022).
In general, all medications that are taken during pregnancy should be discussed with your healthcare team, including your obstetrician. Medications that control symptoms and could be considered safer during pregnancy include:
Recommended Heart Rate Controlling Agents
Beta blockers: Propranolol may be continued in pregnancy at 5 mg twice daily, or metoprolol 12.5-25 mg once or twice daily (Morgan et al. 2022).
Recommended Vasoactive and Volume-Expanding Agents
Cholinesterase Inhibitors: Pyridostigmine bromide has been used safely in pregnancy for people with myasthenia gravis for decades. A dose of 30 mg twice daily may help POTS patients whose symptoms worsen during pregnancy (Morgan et al. 2022).
Mineralocorticoids: Fludrocortisone may be continued in pregnancy at 0.05-0.1 mg daily (Morgan et al. 2022).
Vasoconstrictors: Midodrine may be continued in pregnancy at 2.5-5 mg three times daily (Morgan et al. 2022).
Medications to AVOID during Pregnancy
Medications that are generally AVOIDED during pregnancy include
- Ivabradine
- Droxidopa
- Benzodiazepines
- Stimulants including dextroamphetamine (Adderall) and methylphenidate (Concerta) (Morgan et al. 2022).
Non-Pharmacological Management of POTS during Pregnancy
Increase fluid and sodium/salt intake. The 2021 POTS Expert Consensus Review (Vernino et al., 2021) endorses patients consuming at least 2-3 Liters of water per day along with 3-10 grams of sodium from ordinary table salt, salt tablets or electrolyte solutions. Pregnant POTSies should drink at least 2.5 L of fluids and ingest at least 7 grams of salt per day (Morgan et al. 2022). One teaspoon of salt contains about 2.3 grams of sodium. Drinking the first 2 cups of fluids before getting out of bed helps some patients.
Try compression hose, abdominal binders and/or gloves with at least 20-30 mm Hg of pressure to help maintain blood flow back to the heart. Recent research suggests that compression garments for the thigh, buttocks, and abdomen (like bike shorts) give the best therapeutic effect. Maternity waist high compression is best for pregnant POTSies to help increase venous return to the heart (Morgan et al. 2022).
Light exercise. Swimming or using a recumbent bike can help to maintain blood plasma volume, muscle mass, and cardiovascular fitness during pregnancy (Morgan et al. 2022). There are some good isometric, aerobic, and resistance exercises for POTS in the modified exercise protocol from the Children's Hospital of Philadelphia, but don’t push too hard during pregnancy. During the second and third trimesters, avoid exercises laying on your back as pressure from the growing fetus can compress the aorta and inferior vena cava (Morgan et al. 2022). Instead, exercises done while seated or lying on the left side are advisable.
Gluten-free diet. Consider going gluten-free for a month to see if it helps to reduce POTS symptoms. POTS patients have a higher prevalence of Celiac Disease (4% vs 1% background rate) and gluten intolerance (42% vs 19% background rate; Penny et al, 2016). In a survey of 20 POTS patients who utilized a gluten-free diet for >4 weeks, the self-reported reduction in POTS symptoms was a whopping 45% (Zha et al., 2022).
Intravenous fluids. 1-2 Liters of fluids administered over 1-2 hours can help to increase blood volume. It is best to use a peripheral vein, if possible, as central lines and PICC lines increase the risk of blood clotting and infection, particularly during pregnancy (Morgan et al. 2022). Check out this page for more information on access routes for intravenous fluids, or this page for administering IV fluids.
Labor and Delivery
Vaginal birth appears to be safe and can be recommended for POTS patients as long as pain control is provided (Blitshteyn et al. 2012) and the birth occurs in a hospital setting in case of complications (Morgan et al. 2022). Intravenous fluids very early in labor can be helpful to minimize low blood pressure (Corbett et al. 2006). Slow titration of epidural anesthesia is recommended to prevent significant blood pressure changes. Giving the epidural early in labor is recommended to prevent pain, a trigger of both autonomic instability and tachycardia (Corbett et al. 2006).
If hypermobile Ehlers-Danlos syndrome is present, there is an increased likelihood of delivering within several hours from the start of contractions. Spontaneous rupture of membranes is more common in this population and can lead to excessive bleeding. Therefore, the medical team needs to be monitor blood loss during delivery closely and be ready to assist if necessary (Morgan et al. 2022).
Diagnosing POTS during Pregnancy
Diagnosing POTS during Pregnancy
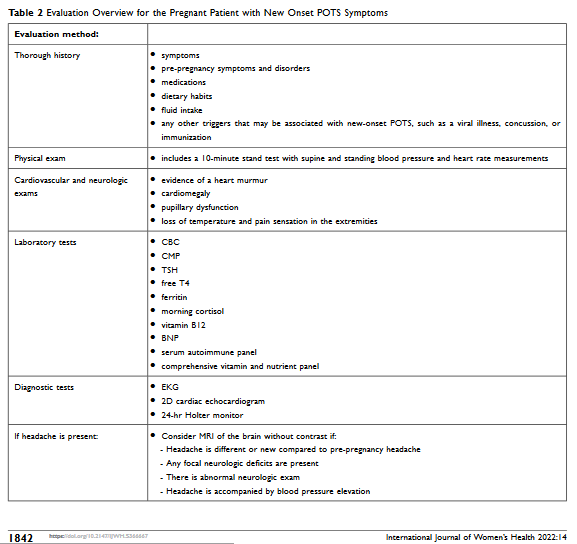
Pregnancy can be a trigger for new onset POTS. In fact, 9% of POTSies believe that their POTS was triggered by pregnancy (Shaw et al. 2019). Evaluation and treatment of a pregnant person with new-onset symptoms suggestive of POTS need to be considered. This table, taken from Morgan et al. 2022, represents the history and testing that Dr. Svetlana Blitshteyn, a top POTS physician, recommends for her own POTS patients.
Table 2. Evaluation Overview for the Pregnant Patient with New Onset POTS Symptoms (taken with permission from Morgan et al. 2022)
Thorough history
- Symptoms
- Pre-pregnancy symptoms and disorders
- Medications
- Dietary habits
- Fluid intake
- Any other triggers that may be associated with new-onset POTS, such as viral illness, concussion, or immunization
Physical exam
- 10 minute stand test with supine and standing blood pressure and heart rate measurements
Cardiovascular and neurologic exams
- Evidence of a heart murmur
- Cardiomegaly
- Pupillary dysfunction
- Loss of temperature and pain sensation in the extremities
Laboratory tests
- CBC
- CMP
- TSH
- Free T4
- Ferritin
- Morning cortisol
- Vitamin B12
- BNP
- Serum autoimmune panel
- Comprehensive vitamin and nutrient panel
Diagnostic tests
- EKG
- 2D cardiac echocardiogram
- 24 hour Holter monitor
If headache is present:
- Consider brain MRI without contrast if:
- Headache is different or new compared to pre-pregnancy headache
- Any focal neurologic deficits are present
- There is abnormal neurologic exam
- Headache is accompanied by blood pressure elevation